DUBAI: There are typically four phases in vaccine trials. The first 3 are the most crucial. That, in theory, is the journey taken all the vaccines against COVID-19. Here, we focus on the journey of Moderna’s mRNA-1273 shot.
First the good news: The clinical trials drew a lot of altruism, with tens of thousands of volunteers who offered their bodies to test the experimental vaccines. In July 2020, at the end of Phases 1 and 2, it already involved hundreds of volunteers. On Monday (November 16, 2020), Moderna’s announcement stunned the world: a 94.5% vaccine efficacy, based on interim data, is as good as can be.
READ MORE
In terms of the data science, the Phase 3 trials followed standard protocol involving 30,000 volunteers. But the trial and analysis aren’t completed yet, though initial results take the mRNA shot closer to getting a licence. If so, it would be the first use in humans of this revolutionary new therapy, altogether changing more than 200 years of vaccine-making process.
Vaccine journey
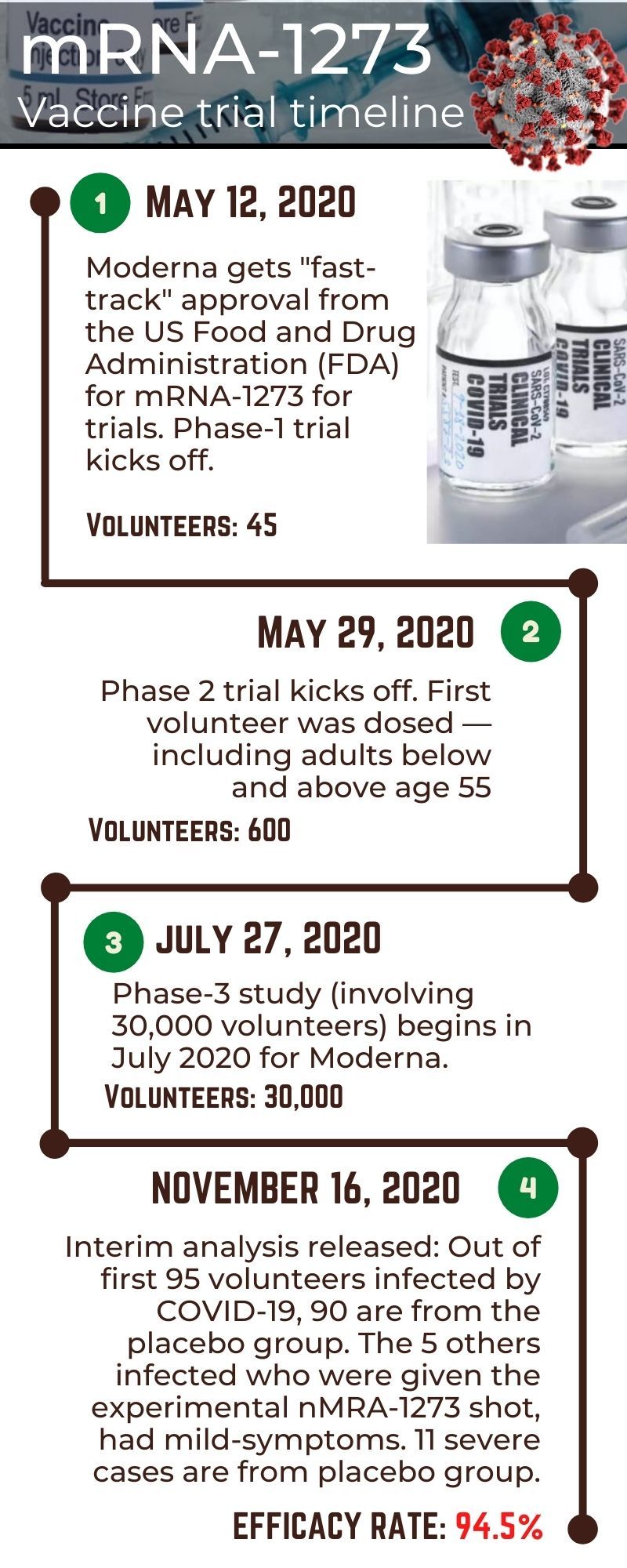
The whole journey took about six months, instead of four to 16 years for a traditional vaccine development route. On May 12, 2020, following animal trials, Moderna received fast-track approval for human trials, from the US Food and Drug Administration (FDA). Phase 1 involved 45 volunteers. A few days later, on May 29, the first volunteer under Phase 2 was dosed, this time with up to 600 participants — including adults below and above age 55.
It ran for two months. Then on July 27, 2020, the Phase-3 study (involving 30,000 volunteers) kicked off. The first “interim analysis” came on November 16, 2020, which showed “94.5% efficacy”:
95 people infected
Moderna, working under the supervision of FDA regulators, stated that out of 95 volunteers infected by COVID-19, 90 had placebo shots. The 5 who were given the experimental nMRA-1273 shot only had mild or moderate symptoms of the viral disease. And of the 11 volunteers who suffered severe COVID-19 cases, all 11 were from the placebo group.
Why is this significant?
First, because there’s a massive number of COVID-19 cases in the US. A research like this can only be beneficial in a geographical area where there’s plenty for cases being naturally transmitted in the community. Add to this the good mix of enthicities in America.
Second, it’s a “double-blind” and extensive research. That means neither the vaccine volunteers nor the vaccine administrators knew whether the experimental shot (with the active mRNA1273 substance) or a placebo (sugar or saline solution) was given. The two shots were made looked identical.
Image Credit: AFP
Third, the assignment of volunteers to either the active vaccine or a placebo was totally randomised. There was no particular sequence, or algothirm used in assigning the shots.
Finally, the recruitment of 30,000 volunteers — from different classes, ethnicities and communiteis — means the results of be statistically significant. Over time, some of the volunteers got sick with COVID-19. To get a preliminary sense of how the trial was going. This is the so-called “gold standard” of clinical research on vaccines and drugs.
How ‘94.5% effectiveness’ came about
An independent board of experts supervised by the FDA checked the data on the first 95 participants who were infected with COVID-19. The result: 90 of the initial 95 volunteers who were infected with COVID-19 received the placebo. Only 5 had been given the experimental mRNA-1273 vaccine. Based on that data, the board estimated that the vaccine is 94.5 per cent effective.
What does it prove?
It suggests that mRNA vaccine, the platform used by both Moderna and Prizer (also by CureVac), can help the world break free from the grip of COVID-19. A whole generation of scientists had been working on mRNA therapies — testing it to treat everything from tumors to degenerative diseases. If the mRNA-1273 and Pfizer’s BNT162-b2 shots are approved, it would be the first time mRNA technology would be authorised for use in humans, and that too, on a massive scale. But more than this, it represents a revolution in vaccine development.
Why is it revolutionary?
For 224 years (from 1796) from the time British doctor Edward Jenner first used a real virus to treat smallpox, vaccines always involved the use of a real virus — in one form or another (live “attenuated, “killed” inactivated, sub-unit, recombinant, conjugate, etc). mRNA does away with that. It also speeds up the process.
Traditionally, vaccines take time to develop, typically 16 years (fastest was four years). mRNA speeds up this process. In effect, it turns vaccine development into software programming, using DNA sequencing to enhance the human body’s own machinery to do exactly what the body does once infected.
With mRNA, scientists make use of supe computers to conduct what amounts to genetic engineering — the manipulation of cells at the genetic level. mRNA is seen as the advanced biopharma industry’s answer to a whole new class of pathogens — or infectious agents — for which no specific vaccines exist yet. Going forward, experts like Dr Ugur Sahin, 55, inventor of Pfizer’s mRNA vaccine, believe could the mRNA technology can be used to speed up vaccine trials against other infectious diseases in the future.
While administered like other vaccines — via an intramuscular injection — an anti-viral messenger RNA uses synthentic genes. The shot, wrapped in an oily bubble, injects synthetic genes “programmed” to use the human body’s own proteins to generate “fake” viruses similar to specific components of a target pathogen (like the “spike” exo-protein of the SARS-CoV-2) — which then trigger a response from our own immune system.
The bubble can fuse to a muscle cell and deliver the RNA. That molecule is coded with instructions for building a coronavirus spike protein. When a vaccinated cell releases copies of the spike protein, the immune system learns to make antibodies against it.
When do I get the vaccine?
First, the trials (there are 24 vaccines now in Phase 3 stages) need to be completed, as more data from large studies must be gathered to validate the interim data.
Second, the vaccine makers must apply for emergency-use authorisation and health regulators must be fully convinced of their safety and efficacy for any approval to be given. With the COVID-19 candidate vaccines, there’s a lot more work to be done. Moves are afoot to tackle distribution challenges. Airlines and logistics companies will surely be involved in this massive global exercise.
On Tuesday, Pfizer has announced the launch of a “pilot delivery programme” for its BNT162b2 vaccine in 4 US states. The company said the move is to prove distribution routes in the US and other parts of the workd. Events leading to the approval and distribution are sure to draw global attention.
Moderna Inc said its experimental vaccine does not require ultracold freezing, a factor that could prove to be major advantage over Pfizer’s product.